The Overdose Epidemic
We should be marching in the streets over the state of opioid use disorder treatment.
Responding effectively to the Opioid Overdose Epidemic
The epidemic of accidental opioid poisoning has received increasing media coverage as opioid-related deaths have skyrocketed. But the magnitude of the problem is still largely unappreciated. The New York Times
recently illustrated that annual drug-related mortality in the United States has surpassed peak annual deaths related to AIDS, gun violence, and car accidents. What’s most troubling is that the rate of opioid-related deaths is rising faster than ever.
At the height of the AIDS epidemic, activists used rallies, marches, “die-ins”, and other targeted “actions” to draw media attention to the human cost of the AIDS epidemic. A primary complaint was that the FDA wasn’t getting experimental medications to market fast enough. Through creative and persistent protest AIDS activists fundamentally changed the way that the FDA approves new medications.
When effective antiretroviral medications were discovered, AIDS-related mortality plummeted even as the number of persons living with HIV and AIDS continued to climb.
. HIV Surveillance--United States, 1981-2008")
There are several similarities between AIDS and Opioid Use Disorder (OUD).
- The illnesses are contracted through environmental exposure--AIDS through exposure to the human immunodeficiency virus and OUD through exposure to highly potent opioid drugs;
- Exposure is most often mediated by human behaviors--AIDS by sexual intercourse and IV-drug use and OUD by recreational or medical opioid use;
- The illnesses typically spread peer-to-peer;
- The illnesses, if untreated, are highly lethal; and
- Once contracted, the illnesses are typically chronic and require maintenance treatment to prevent progression and death.
There is at least one glaring difference between the AIDS and OUD mortality crises. AIDS caused record annual deaths just before effective medications were discovered and brought to market. OUD is currently contributing to record mortality rates even though life-saving medications (methadone and buprenorphine) have long been FDA-approved and marketed to providers. Methadone was FDA-approved for OUD in 1972 and buprenorphine in 2003.
What’s the catch? As of March 31, 2016, 82% of facilities that treat addiction provided outpatient treatment, but only 21% provided outpatient methadone or buprenorphine maintenance. For that reason, only a minority of persons with OUD are provided the two maintenance pharmacotherapies known to drastically decrease their morbidity and mortality risk. If pharmacotherapy for OUD were implemented as widely as antirotroviral therapy for HIV/AIDS, we would save tens of thousands of lives and begin to reverse the epidemic of opioid-related deaths.
Readers may contest the claim that medical treatment would reverse the overdose epidemic. The claim can only be tested empirically by increased access to medical treatment; but the research support for this approach is overwhelming. Consider the most recent meta-analysis of treatment cohorts, including more than 120,000 methadone patients and more than 15,000 buprenorphine patients. The methadone cohorts were followed between 1 and 13 years and the buprenorphine cohorts between 1 and 5 years. When patients were undergoing maintenance medical treatment, their all-cause mortality rates were two (buprenorphine) and three (methadone) times lower than when they were out of treatment.


Sordo, Luis, et al. "Mortality risk during and after opioid substitution treatment: systematic review and meta-analysis of cohort studies." bmj 357 (2017): j1550.New Paragraph
This type of analysis assumes that OUD is chronic medical condition like diabetes or heart disease and that craving drives the progression of the illness. Just as we treat hypertension because it drives the progression of heart disease, we treat craving because it drives the progression of OUD. Medications for chronic conditions work when a patient is taking them and stop working when treatment is discontinued.
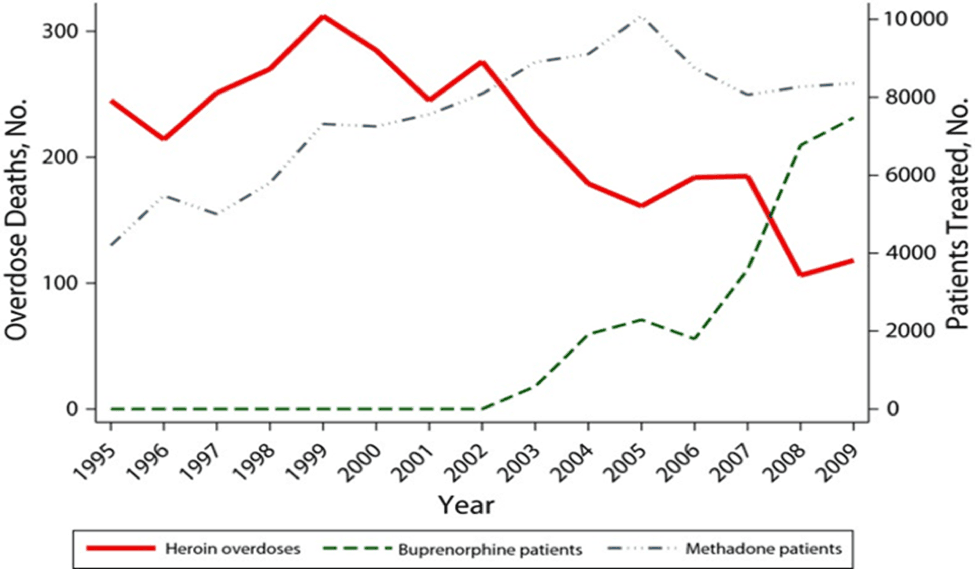
The correlation between increased buprenorphine treatment and decreased overdose death has been observed in both France and Baltimore following government-sponsored initiatives to support buprenorphine treatment access.
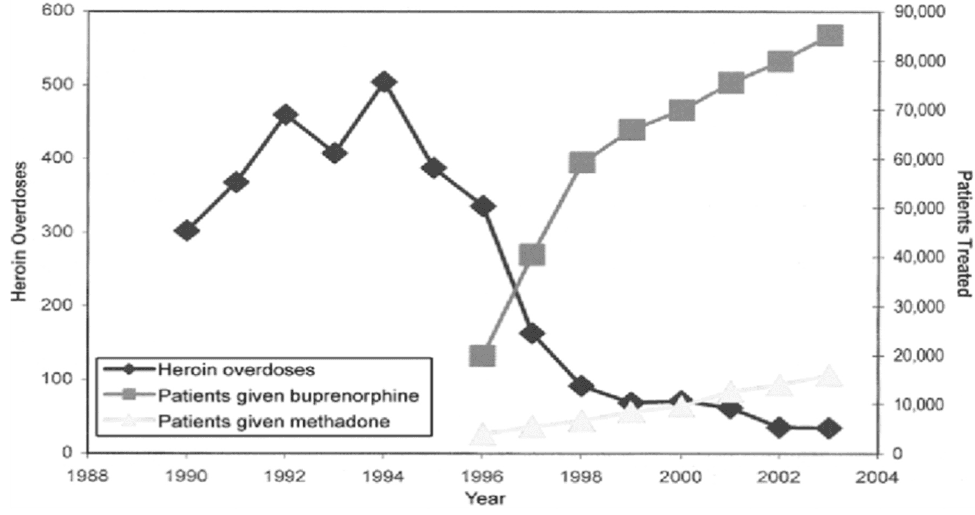
Carrieri, Maria Patrizia, et al. "Buprenorphine use: the international experience." Clinical Infectious Diseases 43. Supplement 4 (2006): S197-S215
Schwartz, Robert P., et al. "Opioid agonist treatments and heroin overdose deaths in Baltimore, Maryland, 1995–2009." American journal of public health 103.5 (2013): 917-922.New Paragraph
AIDS activists were taking to the streets to get experimental (and often ineffective) medications to market faster. Drug and alcohol treatment providers fail in a large majority of cases to deliver effective and often life-saving pharmacotherapy to persons with OUD. The rate at which persons diagnosed with OUD are denied effective medical treatment has no comparison among other potentially fatal medical conditions.
This gap between evidence and practice is not unprecedented in behavioral health. Even scientists established the effectiveness of depression medication, many prominent treatment centers refused to provide medication to their patients suffering from depression.
As detailed in a recent article by Luis Guiffra, MD, the tide turned when one prominent treatment center was sued by a former patient for malpractice. 41-year-old Raphael Osheroff enrolled at Chestnut’s Lodge for depression, anxiety, and suicidality. For seven costly months, he was treated unsuccessfully with psychodynamic psychotherapy. After transferring to a medical treatment center, he was provided medication and his condition improved rapidly. In a landmark malpractice case, Osheroff and Chestnut Lodge settled for an undisclosed amount, and the treatment center eventually shut its doors. Dr. Guiffra argues that the field of OUD treatment is ripe for legal action against treatment centers that ignore science in favor of tradition, denying patients effective, often life-saving treatment.
The “opioid crisis” has attracted a huge investment of money for prevention and treatment. But it may be that we could achieve the most important gains by using the money we already have more effectively. This blog series will attempt to provide pragmatic, evidence-based guidance on how we can achieve the goal of reversing the overdose epidemic. Topics will include:
1) Reducing barriers to effective medical treatment for OUD
2) Changing the organizational and business structures that disincentivize maintenance medical treatment
3) Challenging the cultural bias that favors detox and extended-release naltrexone over maintenance agonist treatment
4) Understanding science to build integrated, evidence-based models of care
We have the resources we need to treat OUD effectively. By implementing them widely and consistently we can revolutionize the standard of care and reverse the overdose epidemic.